Ablation is performed based on the knowledge that atrial fibrillation is always started by extra beats, known as extrasystoles, from certain areas in the atria, typically the pulmonary veins. The general rule of thumb is that you cannot have atrial fibrillation without extrasystoles, however extrasystoles don’t necessarily initiate the onset of atrial fibrillation.
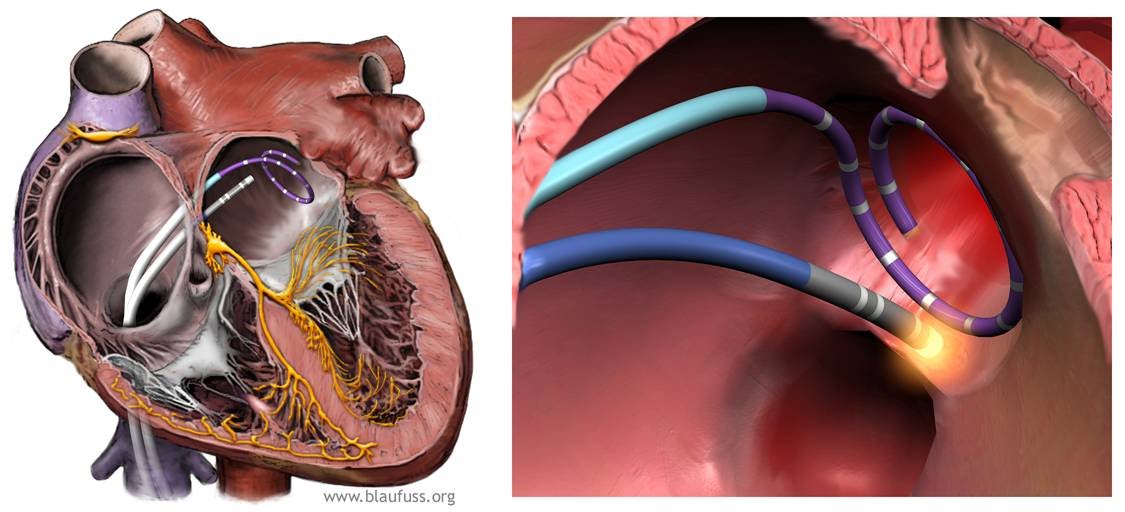
An ablation is performed with a small instrument called an ablation catheter, which is inserted into the left atrium via the vascular system from the groin. Your physician will check whether the ablation has been effective using another small instrument called a circular catheter or a lasso catheter.
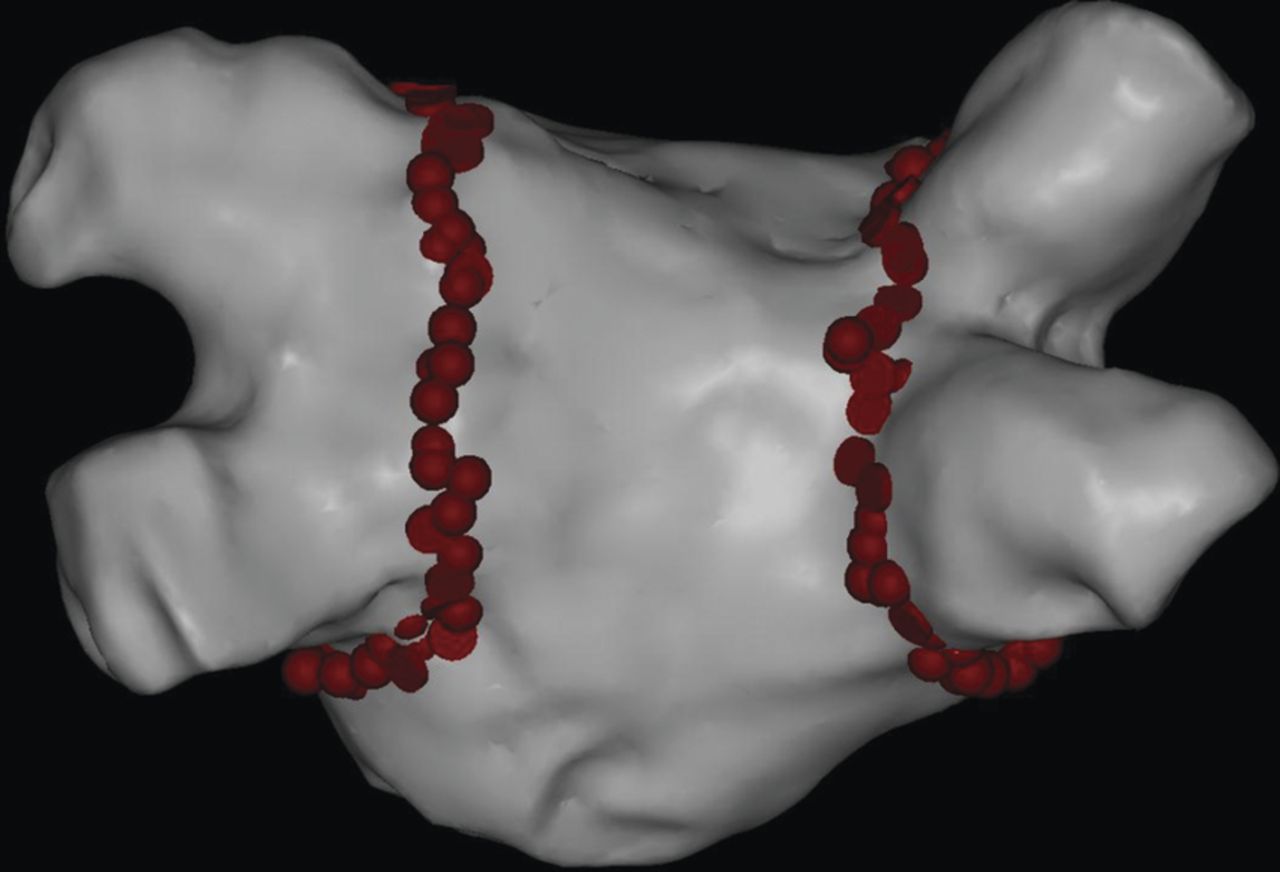
I have created the following image that demonstrates where each ablation is delivered as marked by the red circles. They are overlaid on a picture of the left atrium, with the four pulmonary veins protruding to the left and right sides respectively.
During the ablation process the patient’s heart musculatore is heated up to approximately 65 to 70 degrees centigrade (149 – 158 fahrenheit). This burns the muscle cells, causing a scar where the heat was applied. This scar forms a barrier to the electrical impulse line which does not allow electrical impulses from inside the ablated areas to escape to the rest of the heart musculature.
If the ablation is performed correctly there will be a scar around the sources of extrasystoles. This will prevent the extra beats from disturbing the normal heart rhythm, preventing the onset of atrial fibrillation. The same effect can be achieved by freezing the tissue in a procedure known as cryo-ablation.
Does Ablation Treatment Damage The Heart?
In short, Yes – that’s actually the whole point of it. In latin ablatio means “cut away; remove”. However we aren’t hacking away randomly at the heart, this treatment has been perfected over more than 20 years and it does not affect the functioning of the atria. The target areas of ablation treatment are not involved in the emptying function of the atria to any measurable degree.
This doesn’t mean that the treatment is without risk. It is important that the heat, or cold if cryo-ablation is used, only affects the atrial tissue and doesn’t damage other organs or structures. If ablation is performed improperly it could damage the pulmonary veins, the esophagus, the phrenic nerve, or the lungs. It is also important that the temperature is controlled so that a hole is not burned through the atrial wall, which would cause bleeding into the heart cavity.
This means that it is important that the procedure is performed in a controlled manner. This maximizes the chance that an effective barrier is formed, while limiting the risk of harmful side effects as much as possible. Essentially your physician is trying to strike a good balance between high (or low) temperatures while minimizing risk.
The downside of this necessary caution is that occasionally not enough tissue is burned to create a lasting effect, creating holes in the “barrier”. This means that the chaotic impulses which start atrial fibrillation may occasionally find their way into the heart, which means that the patient may still get atrial fibrillation.
Multiple ablation treatments might be necessary
In these cases it may be necessary to repeat the ablation treatment. This is necessary in about 15-20% of cases within the first year of treatment. 5 years ago this figure was as high as 35-40% so ablation treatments are clearly becoming more effective as we become more experienced in performing them.
The important takeaway is that there are very low risks of adverse side-effects to an ablation treatment. In experienced hands the risk for serious side effects or complications to ablation for atrial fibrillation may be well below 1%.
The first weeks after ablation treatment
In the first weeks – up to three months – after undergoing ablation treatment, atrial fibrillation may continue to occur. It can even surprise patients by occurring just after they have undergone surgery.
This is because the operation itself stresses the heart. Typically when the heart is stressed it is more prone to developing atrial fibrillation. This is also true regarding other heart operations. For example if you replace a heart valve or perform a bypass operation.
This does not always happen but it can sometimes be very unpleasant. The episodes will usually occur over the course of a few weeks. If a patient experiences particularly bad episodes in the first few weeks after ablation, I would often recommend that they undergo a course of antiarrhytmic medication – e.g. amiodarone/Cordarone – for the first few months.
This is also the reason why your physician often recommends continuing with your regular medication for a period – often the first three months – after undergoing ablation treatment.
Which Factors Impact Ablation Treatment?
Ablation treatment is typically more effective if the patient has a periodic flicker than if atrial fibrillation is constantly present. This is due to the fact that constant AF can cause permanent changes in the heart muscle, which themselves increase the risk of AF. Patients can still undergo ablation treatment if they have constant AF, but should tone down their expectations for the result.
This means that it is important for patients to take early action when they experience a constant flicker. Unfortunately doctors have a tendency to try to exhaust all options for treatment with medication before proposing ablation treatment. This caution is typically unnecessary, and there is growing evidence for referring patients to ablation treatment earlier.
If you feel that your quality of life is significantly affected by your atrial fibrillation, despite the medication you are given, you should not feel afraid to push for a referral for ablation treatment. The same is true if you are experiencing significant side effects due to the medication you are receiving.
How Can I Help Improve The Results Of My Ablation?
We know that patients who are significantly overweight or have sleep apnea are both at an increased risk of getting atrial fibrillation, or having AF reoccur after an ablation treatment or medical treatment. It is therefore important to try to maintain a healthy weight and to undergo treatment for sleep apnea if necessary.
Contrary to some physicians I do not think there is any compelling evidence to recommend abstaining from, for example, coffee and moderate amounts of alcohol. There is also no evidence confirming that certain types of diet should be avoided – or are beneficial.
We have compiled a guide with more information here:
Can Ablation Treatment Completely Eliminate Atrial Fibrillation Symptoms?
There are convincing evidence that shows that ablation treatment gives good results if medicine was not effective. There are also several studies demonstrating that ablation treatment has a greater chance of providing stable and normal heart rhythm than medical treatment. Some studies have shown that more than 80% of patients do not have atrial fibrillation for 5 years after an ablation treatment. These studies also show that less than 10% of these patients need additional rhythm-regulating medication. To achieve these results more than one treatment may be needed.
Ablation Is a Low Risk Treatment With Good Results
Ablation for atrial fibrillation is a treatment with high expectations of being able to restore a normal heart rhythm in people otherwise very bothered by their atrial fibrillation. The treatment has a low risk of complication when conducted by experienced physicians.